Resources
Identifying the Value of Computers in Dialysis
Part I: Business Applications
John A. Sargent, PhD
Introduction
Over the past few decades, computers have been increasingly used in most areas of business, and their application to various dialysis activities—including “renal management systems”—is no exception. It should be noted, however that in whatever context computers are used, they are merely tools that can help with complex tasks.’ Renal management systems fall into two broad categories—business systems and clinical systems. The dialysis industry has used computers effectively in many aspects of the non-clinical part of its business. The use of computerized clinical systems, however has lagged. Over the past decade there have been mixed reviews regarding whether this technology has had an impact on the conduct of the treatment itself. There has in fact been a general acceptance of other technological improvements in dialysis (for example, microprocessor-driven dialysis machines), but dialysis providers have not universally adopted the use of computers in guiding the delivery of clinical care.1
Typical goals of introducing computerization into virtually any field are:
- to automate complicated, repetitive tasks and ease staff burden
- to develop knowledge and understanding of an operation so that it can be conducted in a more effective manner
Defining the Problem to Develop the Solution
It may seem obvious that a problem should be defined before a solution is attempted. However, the rapid expansion of computer capabilities has led to the view that if one collects a large amount of data, the answers to problems—some that haven’t even been identified—will appear. Some in the computer and business fields have recognized that much data collection and computerization are apparently done for their own sake— it is, after all, very easy with modem technology.2—4 However, the problem is that a vast increase in data, without a guiding reason behind collection of that data, results in no greater understanding (knowledge). Walter Wristen has pointed out the paradox of the use of information technology:
“The incessant production of new data and their instantaneous communication create a paradox: Information, the thing that eliminates uncertainty, now increases everybody’s feeling of insecurity because of the failure to convert data into knowledge.” 4
With the small operating margins in dialysis and the potential increased operating cost that computerization represents, it is critical to make sure that systems are addressing a defined and important problem. The keys to getting benefit out of renal management systems are:
- to clearly define what understanding (or knowledge) is desired
- to determine what information is needed to gain that understanding
- to select the data that need to be collected to generate that information
This process—moving from the definition of the knowledge desired to the data to be collected—vastly reduces the amount of effort and data that need to be collected and processed. It can also control the cost of the resulting technological solution.
Evaluating the Cost and Benefits of Dialysis Computer Systems
The cost of operating computerized systems
While elements of computer costs will be discussed in detail for various applications below, it should be stressed that costs are not trivial and are not solely the cost of hardware and software. Computerization involves the entire organization: staff specifically skilled in the software need to be hired, existing staff need to be trained, and operating routines may need to be changed. In addition, once an application is relied on to perform a function, any disruption can be chaotic; thus, contingency plans must be made for such a possibility. It follows that the value of automation should be great enough to warrant these costs.
Computerizing easily defined/tedious tasks versus analytical applications
Of the two categories of computerization described above, automation of complicated, repetitive tasks is the most obvious application and the one that is the easiest to define. Examples of computerized functions in this category are payroll, general ledger and accounting systems, and most renal business systems. In contrast, developing knowledge and understanding of an operation, such as improving clinical care, involves analysis of several functions and is a much more difficult task.
Establishing the overall goals for computerization
In setting goals for computerization one must take care to concentrate on the problem of interest, not the mechanism—the means of collecting and storing data. Examples of a “problem of interest” are how to reduce receivables in the business setting or how to track and evaluate blood access problems in a dialysis clinic. The unsophisticated potential user may see data collection and storage as the goal and may lump it together with the need for a “paperless” enterprise. This approach probably results from the use of manual data collection methods that, in many cases, lend themselves to automation. However, it is often not paper itself that is the problem but rather the inability to retrieve specific pieces of information without sifting through large amounts of recorded data. Paper is attacked not because it is paper but because the information it contains is a mixture of the useful and the trivial. Putting all of those same data in a database can help, but it merely moves the same mixture of useful and trivial data to an electronic storage medium.
The real goals of computerization should concentrate on desired results. Goals should include:
- automating complicated tasks—billing, accounts payable, payroll
- assuring complete charge capture of treatment items
- easing staff burden by:
- eliminating data copying
- producing analyses for controlling agencies
- making information useful
- making better use of clinical information
- anticipating problems and assuring that critical problems are being addressed
Determining the value of computerization
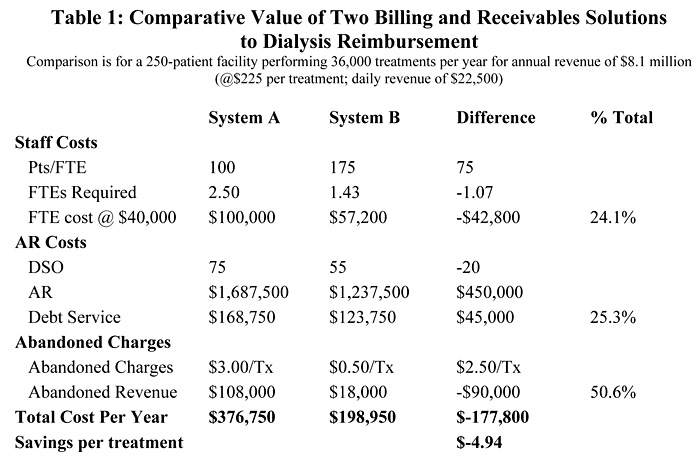
To determine the value of computerization, one has to quantify the value of the specific goals. Some valuations are easier than others, such as the value of decreasing accounts receivable.5 For example, for a 250-patient enterprise (36,000 treatments per year; $8.1 million annual revenue; $22,500 per day) a typical provider could have 75 clays of revenue ($1,687,500) not yet paid (days service outstanding, DSO). Increasing the speed of collections and reducing that number by $450,000 to $1,237,500 (55 days DSO) would yield $450,000 at an annual debt service of $45,000 ($1.25 per treatment). Other tasks, such as being able to ease staff burden or anticipate problems, are more difficult to quantify.
Nonetheless, to be able to evaluate the extent to which computerization is justifiable, some estimate of the value of each of the candidate goals should be made.
How Does the Dialysis Facility Pay for Computerization?
The dialysis provider has been in a tight financial situation for many years. Even with the recent increase in the composite rate, operating margins are small. As a result, the dialysis provider doesn’t have the luxury of avoiding the question, “How are we going to pay for computerization?” The answer is relatively simple. There are three options:
- Increase revenue by computerization. Increased revenue with effective means to capture charges, to reduce abandoned charges (the ones that are viewed “not worth pursuing” when denied), or increasing the number of treatments delivered and billed for.
- Decrease in costs by computerization. Costs can be decreased through more effective administrative and/or clinical staff (i.e., reducing the personnel per unit of service), reducing operating costs (such as lower debt service due to reduced level of receivables, as described above), or some other efficiency that has a financial impact.
- Increase the cost of doing business. This option says, “We need computerization. It won’t increase revenue or decrease cost, or if it does, it won’t pay for itself However, we need it so it will be a part of our overhead costs.”
Using a “Business Problem” Analysis
Many business applications readily lend themselves to the type of definition and evaluation that should be done as the dialysis provider considers computerization. There are several business systems that fall into this category and many of them are common to virtually all businesses. For example, accounting systems to record invoices and generate payments are universal. So too, is the general ledger, with rules that have been defined for centuries. Systems for these applications are readily available and a wide range of these systems can easily be adapted to dialysis. The billing and accounts receivables problem for dialysis, however, is unique. It is unique because of the regulated nature of dialysis and the complex reimbursement rules which govern claims, insurance coverage, charge justification, claim formatting, etc. Thus to illustrate the process for defining and evaluating a computer application for its value to the dialysis field, it is useful to focus on an analysis using billing and accounts receivable management as a well defined subsystem of the “Renal Business Management System” before moving on to the evaluation of more complex clinical systems.
Defining the Need for Billing and AR Systems
Dialysis providers need to submit claims for services to appropriate payers and, in most cases, in compliance with complex rules resulting from regulations, such as government requirements or negotiated contracts with private payers. The challenges for dialysis providers in the billing operation are:
- to control staff costs for the task of bill production and collections
- to assure complete billing for all services
- to reduce the number of charges that are written off as uncollectable or not worth pursuing
- to assure rapid and complete collection of amounts owed so that large amounts of the provider’s money do not remain uncollected and that debt service (the interest on money borrowed, which is reduced if more receivables are collected) is minimized
These goals can be used to define the desired attributes of a system to address the billing/AR problem:
- To reduce staff costs, the system should be easy to use and directly address the complexity of the dialysis problem so that “work-arounds” are minimized.
- To assure complete billing, the system should have mechanisms to check entered charges against orders, and methods of determining which charges are correct when discrepancies are found.
- To reduce abandoned charges, the system should have an easy method of making corrections and rebilling contested charges, as well as a method to delete a bill and make all associated accounting adjustments when the wrong payer is initially billed.
- To minimize accounts receivable, the system should have collection tools and tracking reports to help staff pursue amounts owed in the most efficient manner.
Defining the Value, Cost, and Benefit of Automation
Figure 1 illustrates the approach to this analysis. This figure shows that there are costs associated with two aspects of the problem of automation for most processes:
- the system cost (curve A in Figure 1)
- the cost of the function or operation that is the goal for computerization (curve B in Figure 1)
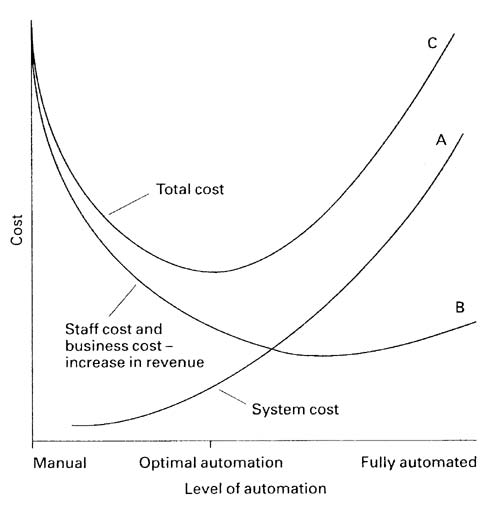
Figure 1
The cost of the system is a combination of the actual purchase price and the ongoing costs of running the system, plus the cost of using the system. System costs include support costs and internal staff costs that are outside of vendor expenses; these costs will increase with the complexity of the system as the general system user routinely accesses less of the overall system and more specialized knowledge is needed.6 It would be assumed that as the system becomes more complex it does so because it has features that make it more useful and better able to meet the goals that have been outlined for its use. It should be noted that if the increased complexity is the result of collecting and storing all data whether or not it is useful or trivial, this added cost may have little or no benefit.
The cost of the function as it is computerized is shown in Figure 1 as curve B. As the system used to address the function becomes more complex, the costs of the functions it addresses should decrease. This is shown as an initial rapid decrease with modest computer complexity (and expenditure) because there are elements of the problem that readily lend themselves to automation. This cost relationship is shown to level off as the system complexity increases to the point where it no longer has much impact. Although there may continue to be a decrease in the cost of the target function, increases in staff costs to operate the system ultimately dominate.
The total cost to the provider is the sum of these two curves, the system cost (A) and the cost of the function (B), (shown as curve C). This cost is seen to reach a minimum, which will be the ideal operating point for the provider. This figure illustrates that computerization without limit does not provide the same benefits as automation to an optimum level. Once again, finding this optimum requires definition of the problems to be solved and selecting a solution that meets those needs.
Analysis and Evaluation of Dialysis Billing and AR Tracking
Virtually no dialysis provider produces claims and tracks receivables by hand. There are many automated systems in use in the field. Some are “home grown,” some are ones that hospitals traditionally use for their acutely admitted patients, some are modifications of systems for another aspect of medicine, and some are designed specifically for dialysis. Table I shows a comparison of systems that represent these last two categories—modification of a system for another medical specialty (System A) and one designed specifically for dialysis (System B). Both systems are in widespread use in the dialysis field.
The functional costs of the two systems
The characteristics of System A are that one staff member (FTE) can handle all aspects of billing and collections for 100 patients; with System B, this number is 175 patients. System B addresses the re-billing functions and the unique nature of dialysis billing and coverage issues, and typically results in DSO of 55 days in contrast to 75 days for System A. The tedium of re-generating claims and general work-arounds required with System A result in abandoned charges of $3 .00 per treatment; with System B abandoned charges are $0.50. The comparison of these two systems shows a combined decrease in billing and collection costs and an increase in revenue of nearly $5.00 per treatment if System B is used in preference to System A.
The system costs
Table II shows a general comparison of three computing systems that would be representative points along the horizontal axis of Figure 1—system complexity. These costs, which have been discussed elsewhere,6 do not relate to any specific system or application but serve to emphasize the elements that are common in the overall cost of a system. It should be noted that as the system becomes more complex, so do all the costs. This can include the need for a Systems Manager, who is the internal “expert” on the system and who is called upon to help with problems, train staff, address system issues internally, etc. Hardware and software purchase price is shown as well as the annual cost for a three-year amortization of the purchase (a reasonable “life” in this rapidly evolving field).
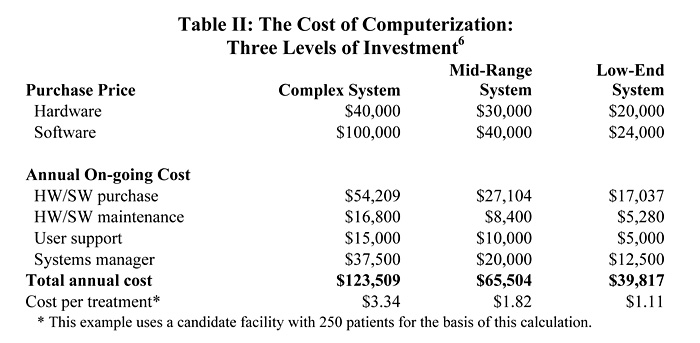
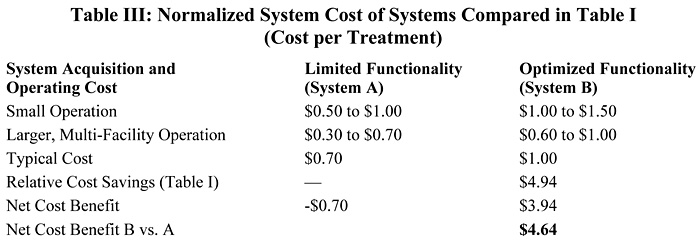
For certain applications, some of the costs shown may be too high. Systems in constant use by a small number of individuals who are completely familiar with the system will need less support and there may be a correspondingly smaller Systems Manager requirement. With these adjustments, and normalizing for a range of facility sizes, the actual costs of Systems A and B are shown in Table III and are less than $1.00 per treatment. The purchase price of System A is about 30% lower than that for System B. The combined analysis, however, as indicated in Figure 1 as the sum of costs, shows that even though System A is “cheaper,” the overall cost of System A is actually higher by $4.64 per treatment because it lacks the specific capabilities that resulted in the $4.94 per treatment savings when using System B.
Conclusion
Computers are effective tools to address complex tasks. To be useful and cost effective, however, the specific aspects of the problems that lend themselves to automation must be defined. Reimbursement in dialysis is such a problem and because of its unique features, as required by regulating groups and payers, well-targeted solutions are required. Other aspects of automation in dialysis, particularly those regarding the collection, storage, and use of clinical data, are not as well defined. The second part of this analysis, to appear next month, will evaluate the capabilities of computers in addressing the effective use of information to improve the clinical care of the dialysis patient.
References
- 1. Sargent JA: Gathering data in the dialysis unit: What do you need? What do you need it for? Nephrol News Issues 13:9:19, 1999
- 2. Kohanski D: Information isn’t knowledge. San Francisco Chronicle September 15, 2000
- 3. Kohanski D: Moths in the machine: The power and perils of programming. St. Martin’s Press, April 2000
- 4. Wriston WB: The world according to Walter. Harvard Business Review 64:1:65, 1986
- 5. Sargent JA: Reimbursement: The fuel for high-quality dialysis care. Contemp Dial Nephrol March 2000, p.21
- 6. Sargent JA, Clark RA, Paget M, Kingston WW: Cost-effectiveness of computer solutions in dialysis. Dial Transpl 20:4, 1991